Pediatirc Nephrology/ Henoch-Schönlein Purpura
ETIOLOGY
Henoch-Schönlein purpura (HSP) is a vasculitis of unknown etiology characterized by inflammation of small blood vessels with leukocytic infiltration of tissue, hemorrhage, and ischemia. The immune complexes associated with HSP are predominantly composed of IgA
Arthritis occurs in 80% of patients with HSP; it can occur in any joint but tends to affect the lower extremities, most commonly the ankles and knees. The arthritis is acute and can be very painful with refusal to bear weight.
Henoch-Schönlein purpura (HSP) is a vasculitis of unknown etiology characterized by inflammation of small blood vessels with leukocytic infiltration of tissue, hemorrhage, and ischemia. The immune complexes associated with HSP are predominantly composed of IgA
EPIDEMIOLOGY
It occurs primarily in children 3 to 15 years of age, although it has been described in adults. HSP is slightly more common in boys than girls and occurs more frequently in the winter than the summer monthsCLINICAL MANIFESTATIONS
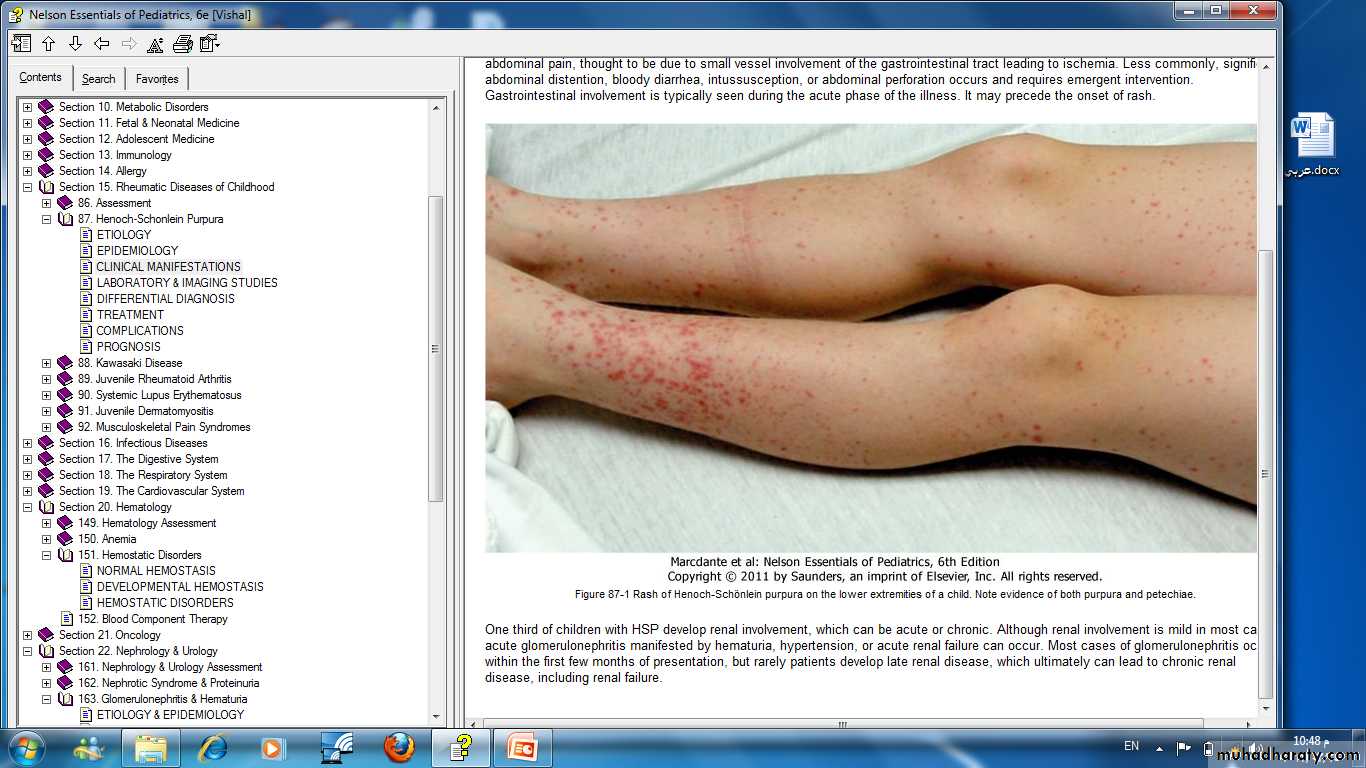
HSP is characterized by rash, arthritis, and, less frequently, gastrointestinal or renal vasculitis. The hallmark of HSP is palpable purpura, caused by small vessel inflammation in the skin leading to extravasation of blood into the surrounding tissues. IgA often is deposited in the lesions. Although the rash can occur anywhere on the body, it is classically, below the waist on the buttocks and lower extremities


Comments
Post a Comment